Introduction
The relationship of Humanity with cannabis spans thousands of years, with evidence dating back approximately 12,000 years. Yet, this connection likely extends even further, as cannabis predates humans, with an estimated age of over 70 million years (Clarke & Merlin 2012). Despite its longstanding and widespread use across cultures, cannabis remains controversial, stirring debates across scientific, social, and ethical spheres—even extending to its nomenclature. In this book, we will focus on its medical applications, briefly touching on relevant collateral topics, while referring readers to other sources for broader discussions.
Since the mid-20th century, research has increasingly clarified the pharmacological mechanisms behind the effects of cannabis, revealing that most are mediated by the endocannabinoid system—a system unknown until then, and still absent from formal medical and biomedical education curricula (see Table 1).
The plant
Cannabis is native to many regions and thrives across a wide range of climates. Since ancient times, it has existed both as a wild plant and as a cultivated one. Its uses are diverse: as a raw material for ropes, fabrics, and building materials (industrial hemp); as an ingredient for medicines (pharmaceutical hemp); and as a plant for recreational or euphoric use. The latter two categories are indicative of the pharmacologically active nature of its substances. While recreational use still remains illegal in several jurisdictions, it has been decriminalized or even legalized in countries like Canada, the Netherlands, Spain, Switzerland, and parts of the United States. The industrial applications of hemp have recently re-gained their legal status in most jurisdictions under certain conditions, though effective enforcement still faces challenges. Over time, as stakeholders become more familiar with regulations, it is hoped that the stigma associated with cannabis will gradually diminish.
Cannabis in Europe
The narrative concerning the of medical use cannabis often begins with William Brooke O'Shaughnessy in 1842. He, a physician formerly based in India, returned to England and introduced cannabinoids as medicine (W. B. O'Shaughnessy And The Introduction Of Cannabis To Modern Western Medicine, https://tinyurl.com/5f7kh8pu). However, French physicians may have predated him. L.-R. Aubert-Roche published his treatise "De la Peste ou Typhus d'Orient" in 1840, which included an essay on treating plague with "hachich" (cannabis). This was based on his experience in Egyptian hospitals during the 1834-35 plague epidemic. Edmond de Courtive, a French pharmacist, created "Hachischine", a cannabis tincture, in the mid-1830s. This work was contested by another pharmacist, Joseph-Bernard Gastinel, before the French Academy of Sciences. This publicity led to cannabis being seen as a panacea. However, its effectiveness was questioned during the 1848-49 cholera epidemic, ultimately curtailing its initial reputation as a cure-all (Guba, 2020).
The latter historical example highlights the importance of evidence-based research and realistic expectations when it comes to cannabis. While it may have potential benefits, it is crucial to approach its use with caution and scientific rigor. The French experience shows that public perception can be easily swayed by hype and that the effectiveness of any substance should be carefully evaluated.
The cover of the first medical book on the therapeutic use of cannabis, published in Paris in 1840. It refers to the medical use of cannabinoid preparations in the years before 1840, demonstrating that the French physician L-R. Aubert-Roche preceded the British physician W. B. O'Shaughnessy as the one who introduced cannabis therapy to Europe (Guba, 2020).
The diverse pharmacological actions of cannabis, combined with the limited number of available medicines at the time, made it a widely used remedy beyond France. In England, the reputable medical practice of W.B. O'Shaughnessy, together with reliable cannabis tinctures prepared by the Smith brothers, and even the favor of Queen Victoria, fostered a climate of confidence around cannabis-based treatments. This reputation soon spread to America, where cannabis remained a mainstream therapeutic remedy up until 1937, when the U.S. Marihuana Tax Act rendered its use financially prohibitive (Wikipedia). By 1961, cannabis was made illegal worldwide under a United Nations treaty, although practical and legal restrictions on its cultivation and use had started in other countries much earlier. For instance, according to contemporary newspapers and scientific literature, the challenges around cannabis in Greece began as early as 1884, for obviously different reasons (Οικονομόπουλος, 2014).
Contrary to modern scientific norms, advocating for the medical benefits of cannabis once carried serious consequences for scientists. This is exemplified by a case in the U.K. where a government official faced prosecution for expressing a scientific opinion in support of cannabis, sparking calls for stronger protections for researchers (Dyer 2009). Equally notable is the long-standing, strict control over cannabis-related medical research in the Western world. While a detailed history of prohibition lies beyond the scope of this book, further exploration can be found in the work of Οικονομόπουλος (2014), ΤO IAMA KANNABH (The remedy Cannabis).
Since 1964, a growing body of research, despite attempts to suppress certain findings, suggests that cannabis, when used appropriately, does not pose significant adverse effects on humans, at least not exceeding those associated with many commonly prescribed pharmaceuticals. Concerns surrounding cannabis primarily focus on its psychoactive component, Δ-9-tetrahydrocannabinol (THC), classified as a psychotropic substance, and a drug of abuse. THC can cause altered perception, disorientation, and memory impairment through its interaction with the CB1 receptor and other neurotransmitter systems, including dopamine, serotonin, and glutamate pathways. Therefore, responsible use is crucial, particularly for vulnerable groups. Cannabis use should be avoided by minors, as it may lead to permanent central nervous system damage and negatively impact cognitive development; all the evidence to date points to this, with the exception of a recent MRI study (Scott et al., 2019), so the issue must remain open. It should also be avoided by pregnant women due to potential adverse effects on fetal brain development and the trophoblast [Grant et al., (2018); Marczylo et al., (2010); Abán et al., (2013) & (2018); Costa et al., (2014), Keim et al., (2024)]. Use during lactation remains controversial due to limited and methodologically flawed studies, further complicated by the ongoing debate surrounding cannabis legalization. In conclusion, "correct" use extends beyond appropriate dosage. It involves a careful weighing of potential benefits against risks. Until we have clearer answers, medical professionals should adopt a cautious approach, prioritizing safety .
The situation after legalization
Legalization/decriminalization
The ongoing wave of medical cannabis legalization across various countries shows no signs of slowing down, despite the continued enforcement of the 1961 U. N. Single Convention on Narcotic Drugs. Similarly, the secondary wave of recreational cannabis legalization or decriminalization appears equally unstoppable. These shifts are influenced by several factors: the steady rise of cannabis activism in Western countries since the 1970s; a growing societal shift toward libertarian views; increasing scientific evidence on the therapeutic potential of cannabinoids; and a strong interest from the pharmaceutical industry, incentivized to develop patentable synthetic cannabinoids.
Prescribing-Distribution-Legal Status
At present, legislation has not sufficiently addressed key issues such as prescribing, distribution, and patient access to medicinal cannabis. Nor has there been a clear, scientifically sound, and universally accepted classification for non-psychotropic cannabis products as health supplements, parapharmaceuticals, medicines, or novel foods. Administrative authorities, meanwhile, have been slow to approve requests for psychotropic cannabis treatments for patients with legal access. This transitional period is somewhat expected, given longstanding prohibitionist biases, the cautious stance of regulatory bodies, and the search for “politically correct” solutions. However, cannabis seems likely to become an established therapeutic option, though inflated expectations may pose a risk, recalling the initial enthusiasm and later disappointment seen in France in the 19th century.
The medical community
The medical community is largely unprepared for this shift, due in part to its inherently conservative nature, but more importantly because practicing physicians have received no formal education on the endocannabinoid system, and cannabis therapeutics, either at the undergraduate or postgraduate level. Without training, physicians are unable to fulfill their traditional advisory role in this area. The need for specialized physician training is both urgent and essential. Currently, for-profit educational organizations have taken the lead, offering a blend of online and in-person courses3. Unfortunately, many of these programs provide only a superficial overview of the endocannabinoid system, often oversimplifying it as “two cannabinoid receptors, two endocannabinoids, two synthesis enzymes, and two degradation enzymes”. While it is natural for a time lag to occur between scientific discovery and its establishment in academic texts, the overly simplistic portrayal of the endocannabinoid system prompts questions. What has happened to the fuller understanding of this complex system (see Table 1)?
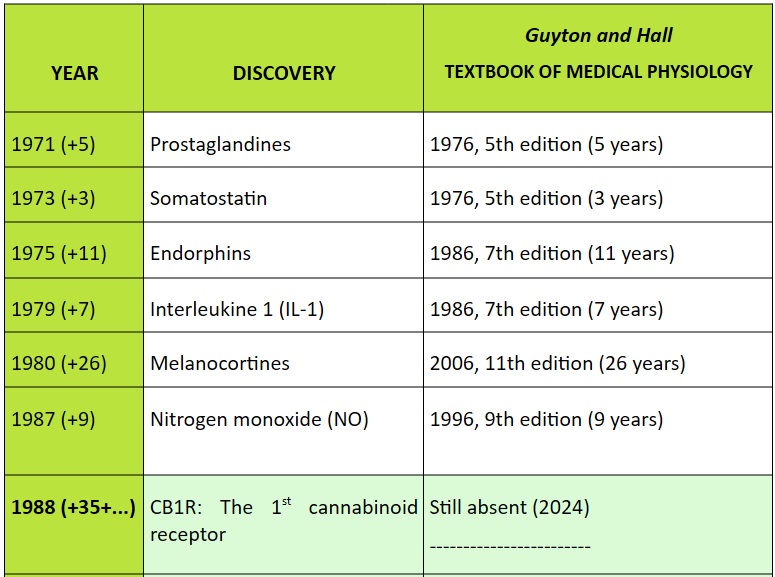

Table 1:Time intervals elapsed from the original publication of various discoveries in the field of physiology, until their appearance in the internationally prestigious textbook "Guyton and Hall - TEXTBOOK OF MEDICAL PHYSIOLOGY" (Hall, J. E., 2020). Based on data collected by Broselid, (2023). The excessive delay of the endocannabinoid-related discoveries is surprising.
The endocannabinoid system is curiously late in becoming a recognized part of standard physiology, despite the abundance of scientific publications that have identified and described it. It's true that the name "endocannabinoid system" is linked to Cannabis sativa L., a plant that has been historically stigmatized. Some researchers believe that this association has hindered the acceptance of the importance of the system in physiology. They argue that the system evolved long before the plant, and that the name creates an unnecessary connection. The suggestion to rename the system to "master homeostatic system". is gaining traction as a way to overcome these prejudices and focus on the system's crucial role in maintaining homeostasis in the body.
The patients
Patients, finding their requests for therapeutic cannabis use unmet by their natural advisors—their doctors—often resort to self-medication. Many of these patients have acquired an impressive level of specialized knowledge. However, it is both clear and undeniable that specialized knowledge, when applied without a foundation in basic science and medical training, can lead to harmful outcomes.
One notable feature of cannabinoids, as compared to other drugs, is their exceptionally high and difficult-to-determine average lethal dose (LD50, or Lethal Dose 50%)5. This trait contributes to their relative safety when used properly. However, driving under the influence of cannabis is an example of misuse and can lead to fatal accidents—especially when cannabis is combined with alcohol, a situation that is unfortunately common. While other drugs and substances have known lethal doses, cannabis’s interactions with them can complicate outcomes significantly. Furthermore, the biochemistry and pharmacology of cannabis therapy are highly complex. Cannabinoids exert their effects primarily through the endocannabinoid system—a system that is both complex and intricately linked with all other bodily systems whose balance it helps regulate [for example: Lipina & Hundal, (2017) on the nitric oxide (NOS-NO) system; Kirkham & Williams, (2001); Chen et al., (2004) on the endorphin system; Ellis et al., (2006) on the orexin system; Morales & Reggio, (2017) on numerous other systems]. Additionally, cannabinoids also act independently of the endocannabinoid system, further increasing their complexity.
To ensure safe, effective, and evidence-based therapeutic use of cannabis, the practitioner should have a solid medical background and specialized training in cannabis pharmacology and clinical application. The long-term interruption of cannabis-related research has disrupted the essential guiding relationship between physician and patient. Restoring this vital relationship requires dedicated education of the medical workforce—a goal this book aims to support.
Therapeutic expectations
The therapeutic use of cannabis is often accompanied by excessive expectations that are not fully justified in practice. This inflated optimism largely stems from the fact that cannabinoid treatments are frequently promoted by individuals without medical training, who, in their simplified view, genuinely believe cannabis to be a cure-all. This belief can even take on a political tone when reframed as the notion that cannabis is the long-suppressed “panacea” denied to patients by “the System.” In reality, while cannabis does have a broad range of therapeutic applications, its effectiveness varies widely by condition, and most uses have yet to be substantiated through double-blind, controlled studies, supplemented by real world evidence. The lack of such research is a direct consequence of the extended prohibition on cannabis. Nonetheless, for many applications still lacking robust evidence, support can be found in traditional medicine across cultures, now partially backed by pre-clinical studies.
A common methodological error in cannabis research is the premature projection of positive results from cell cultures and animal studies onto human subjects, despite the fact that well-documented, human-based studies have not yet been completed. Experience with other drugs has shown that findings in preclinical studies sometimes apply to humans and sometimes do not. Another factor fueling high expectations is that, for many patients, cannabinoids represent a last resort. Patients disappointed by conventional treatments often turn to cannabis with hope and, at times, with a rebellious attitude toward a medical system that they feel has failed them. However, hope and defiance are inevitably accompanied by heightened expectations. A final factor is the widespread promotion of the benefits of cannabis across thousands of websites worldwide. While most of these are driven by legitimate commercial interests, they have led to one of the broadest public disseminations of health information in history. Although many of these sources strive to be credible and carefully cite sources, they often present preclinical study results as though they were directly applicable to humans, which can mislead readers without scientific training.
Regulatory bodies
Conservative stances from official bodies and regulatory agencies have also shaped perceptions, as they continue to uphold outdated or poorly supported views on the potential harms of cannabis. In the United States, for example, many states have legalized or decriminalized cannabis, while the federal government still classifies it as illegal. Governments around the world are passing decriminalization laws, yet the United Nations (UN) only recently downgraded the perceived dangers of cannabis, influenced by a World Health Organization (WHO) report that took a more conservative stance than the current evidence might justify. Medical regulatory bodies like the U.S. Food and Drug Administration (FDA), the European Medicines Agency (EMA), the Greek National Organisation for Medicines (ΕΟΦ) and the like, also struggle to address the unique challenges of cannabinoids, partly due to inconsistent terminology for both the plant and its compounds. This has led to situations where chemically identical cannabinoids are placed in different regulatory categories depending on their source (Riboulet-Zemouli, 2020). Given these challenges, there is a clear need for a specialized cannabis commission with adequate representation from the medical profession, vested with exclusive authority to regulate the therapeutic use of cannabis. Although broader legislative constraints make it difficult to establish an entirely independent body, such a commission could operate within the respective national agencies for medicines of each country and, at the EU level, within the EMA.
Science and Conservatism
Conservative views mentioned above are indeed based on scientific studies, yet these studies often suffer from methodological weaknesses similar to those used to dismiss cannabis research. Examples include: (a) study participants often use other substances (e.g., tobacco, alcohol, psychotropics) in addition to cannabis, (b) sample sizes are typically too small to establish statistical significance, (c) control groups are insufficiently matched to observational groups, (d) cannabis use is often self-reported, without laboratory verification of use levels, (e) studies frequently focus on problematic use but generalize conclusions to therapeutic use, (f) psychiatric studies struggle to separate cannabis effects from genetic, environmental, and social factors, (g) anatomical studies use radiological methods that lack the precision needed to detect specific changes or lesions in the brain, and (h) research rarely distinguishes between varieties of Cannabis sativa L., even though these vary chemically and pharmacologically in a significant way. A related issue is that cannabis strains with higher THC concentrations are increasingly produced for recreational use, which is the primary focus of commercial interest.
In medicine, it is important to avoid turning scientific controversy into a polarized and passionate “for or against” debate. All stakeholders are supposed to seek the scientifically correct position, though their perspectives may differ. Allowing ambiguity to be clouded by emotions, biased arguments, or vested interests ultimately undermines sound judgment. A scientist’s role is to remain objective, forming conclusions based solely on empirical observation and experiment, free from bias, interference, or presuppositions. This neutrality has been absent from cannabis discourse for many years. However, the emotional responses and entrenched divisions around cannabis must now be set aside so we can objectively assess its safety and potential therapeutic benefits for patients.
Moral issues
Some ethicists have expressed concern that patients using cannabis even medicinally may become addicted. However, cannabis ranks relatively low among addictive substances, a fact that is scientifically well-established. It also lacks the serious adverse effects commonly associated with other drugs, particularly opioids, especially when administered under medical supervision. In raising these concerns, ethicists often overlook the following points: (a) the psychotropic effects of cannabis are largely due to only one of its 144 known phytocannabinoids; (b) this psychotropic component is generally not required for treating most conditions; and (c) in cases where it is used, the associated diseases are often severe, incurable, or profoundly distressing, making addiction or psychotropic side effects comparatively insignificant. Notably, many cancer patients are already dependent on opioids (with hopes that cannabis could assist in reducing this dependence), while patients with syndromic epilepsy rely on anti-epileptics, and autistic individuals on anti-epileptic or neuroleptic drugs. In this context, the ethical objection to cannabis use seems more a political and socially charged stance than a medical or moral one, reflecting social hypocrisies that are increasingly difficult to defend. In conclusion, cannabis remains controversial on many levels, including even its terminology (see Chapter 1). The need for medical education on cannabis is pressing and long overdue. Ideally, a single regulatory body should oversee all aspects of cannabis regulation and treatment, consolidating the specialized knowledge needed to manage cannabis as a therapeutic agent—a role for which it does not readily “fit” within conventional pharmaceutical models (see Chapter 2). Academic institutions, particularly universities, should lead the way in funding intensive research to accelerate the move toward evidence-based, widely accepted conclusions. Meanwhile, the endocannabinoid system (see Chapter 3)—a core homeostatic system conserved through evolution from nematodes to mammals—must find its place in standard physiology textbooks.
In the meantime, because people suffering from serious and/or terminal illnesses do not wait for legal or scientific consensus, patients’ right to choose their treatments, whether based on justified or speculative hope, should be respected. Until research reaches greater maturity, patients should not be denied this choice. Ultimately, despite the knowledge gained so far, we still lack actionable insights that can directly guide treatment. If patients seek relief through cannabis, they should be allowed to do so in a coordinated manner, with informed medical advice and oversight from a well-informed medical body, ensuring their choices are respected and supported with proper guidance.
Βιβλιογραφία
Economopoulos, G. (2014). THE REMEDY CANNABIS. (2nd edition., pp. 19–39). Kedros SA (Publishers). Οικονομόπουλος, Γ. (2014). ΤΟ ΙΑΜΑ ΚΑΝΝΑΒΗ (2η έκδοση., pp. 19–39). εκδόσεις Κέδρος ΑΕ.
Abán, C., Leguizamón, G. F., Cella, M., Damiano, A., Franchi, A. M., & Farina, M. G. (2013). Differential expression of endocannabinoid system in normal and preeclamptic placentas: Effects on nitric oxide synthesis. Placenta, 34(1), 67–74.
Abán, C. E., Accialini, P. L., Etcheverry, T., Leguizamón, G. F., Martinez, N. A., & Farina, M. G. (2018). Crosstalk Between Nitric Oxide and Endocannabinoid Signaling Pathways in Normal and Pathological Placentation. Front Physiol, 9.
Broselid, S. (2023). The Missing Chapter: How Human Physiology Textbooks Fail To Include The Endocannabinoid System. Aurea Care Med Sci J. https://aureamedicalsciencejournal.se/the-missing-chapter-how-human-physiology-textbooks-fail-to-include-the-endocannabinoid-system/
Clarke, R., & Merlin, M. D. (2013). Cannabis: Evolution and ethnobotany. Univ of California Press.
Costa, M. A. (2016). The endocannabinoid system: A novel player in human placentation. Reprod Toxicol, 61, 58–67.
Dyer, C. (2009). Scientists want more protection after government adviser is sacked. BMJ, 339(nov04 1), b4563–b4563.
Grant, K. S., Petroff, R., Isoherranen, N., Stella, N., & Burbacher, T. M. (2018). Cannabis use during pregnancy: Pharmacokinetics and effects on child development. Pharmacol Therapeut, 182, 133–151.
Guba, D. A. (2020). Taming Cannabis: Drugs and Empire in Nineteenth-Century France. McGill-Queen’s University Press.
Hall, J. E. (2020). Guyton and Hall Textbook of Medical Physiology E-Book. (M. E. Hall, Ed.). Elsevier Health Sciences.
Keim, S. A., Fried, P., Yeates, K. O., Boone, K. M., Vrantsidis, D. M., Dean, A., Murnan, A. W., et al. (2024). Prenatal Cannabis Exposure and Executive Function and Aggressive Behavior at Age 5 Years. JAMA Pediatr.
Marczylo, T. H., Lam, P. M. W., Amoako, A. A., & Konje, J. C. (2010). Anandamide levels in human female reproductive tissues: Solid-phase extraction and measurement by ultraperformance liquid chromatography tandem mass spectrometry. Anal Biochem, 400(2): 155–162.
Riboulet-Zemouli, K. (2020). ‘Cannabis’ ontologies I: Conceptual issues with Cannabis and cannabinoids terminology. Drug Sci Policy Law, 6, 205032452094579.
Scott, J. C., Rosen, A. F. G., Moore, T. M., Roalf, D. R., Satterthwaite, T. D., Calkins, M. E., Ruparel, K., et al. (2019). Cannabis Use in Youth is Associated with Limited Alterations in Brain Structure. Neuropsychopharmacology, 44(8): 1362-1369
W. B. O’Shaughnessy and the Introduction of Cannabis to Modern Western Medicine. The Public Domain Review. https://publicdomainreview.org/essay/w-b-o-shaughnessy-and-the-introduction-of-cannabis-to-modern-western-medicine/
Wikipedia: Marihuana Tax Act Of 1937. https://en.wikipedia.org/wiki/Marihuana_Tax_Act_of_1937