The following is a clinical excerpt featuring hyperemesis syndromes associated with cannabis use and misuse.
A.10. Cannabis hyperemesis syndrome (CHS)
Cannabis hyperemesis syndrome (CHS) (Chocron, Zuber, & Vaucher, 2019) represents a relatively recent diagnostic category. It was first described in 2004 (Allen et al., 2004) with the report of nine cases presenting with recurrent episodes of vomiting accompanied by nausea and abdominal pain, symptoms that were relieved by very hot bathing. A common background in all cases was prolonged cannabis abuse. CHS has received considerable attention in informational websites concerning cannabis, possibly because it appears paradoxical that a syndrome characterized by severe vomiting may be induced by the same drogue widely used for the relief of nausea and vomiting, for example during chemotherapy. Another striking feature is the relief reported by patients during very hot baths.
With regard to pathogenesis, the hypothesis that tends to prevail attributes the syndrome to a dysregulatory disturbance of hypothalamic function. The hypothalamus plays a central role in thermoregulation and, to a considerable extent, in the regulation of appetite and satiety. It is also an area rich in cannabinoid receptors. The proposed association between cutaneous TRPV1 receptors and the symptomatic relief obtained from hot bathing is particularly attractive, since stimulation of these receptors by heat transmits signals to the hypothalamus (Molinas et al., 2019). These signals are presumed, through mechanisms not yet fully clarified, to temporarily counterbalance the dysregulation that has developed. This hypothesis appears more plausible than the alternative explanation that symptomatic relief results from redistribution of blood volume toward the skin as a consequence of cutaneous hyperemia, with a corresponding reduction of blood flow to the gastrointestinal tract.
This relatively new syndromic entity, which is diagnosed by exclusion, must be carefully distinguished from other dangerous causes of vomiting, as well as from a related condition known as cyclic vomiting syndrome (CVS). CVS comprises a heterogeneous group of underlying dysregulatory disorders, some of which fall within the spectrum of endocannabinoid deficiencies (e.g., migraine, disorders of the autonomic nervous system, etc.). It therefore appears that CHS and CVS are not entirely unrelated entities; rather, additional data are required in order to clarify more precisely the boundaries of each condition (see Figure 20).
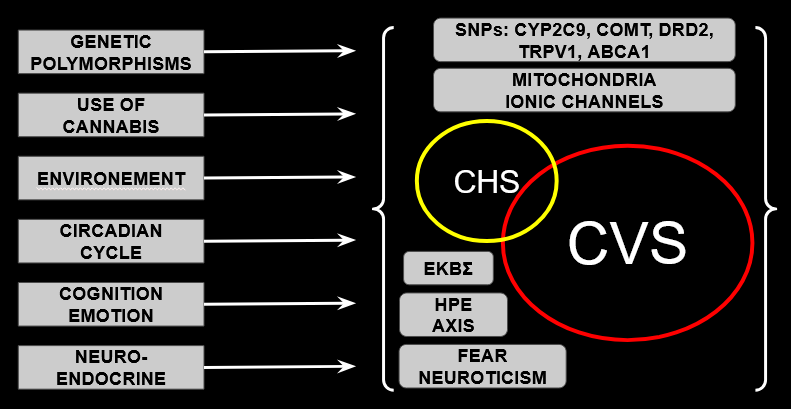
Figure 20. Schematic overview of the presumed pathogenesis and of the relationship between cyclic vomiting syndrome (CVS) and cannabis hyperemesis syndrome (CHS) (Hasler et al., 2019). The Venn diagrams indicate that some cases may be classified either as CHS or as CVS. Various factors are also depicted that may influence, to varying degrees, the manifestation of the two syndromes. CVS: Cyclic Vomiting Syndrome; CHS: Cannabis Hyperemesis Syndrome; ECS: Endocannabinoid System; HPA axis: Hypothalamic–Pituitary–Adrenal axis; SNPs1: Single-nucleotide polymorphisms in the genes indicated.
Diagnostic criteria
The diagnostic criteria currently in use for CHS are the following [Simonetto et al., (2012), modified according to Sorensen et al., (2017)]:
Major characteristics:
• Regular cannabis use for > 1 year (74.8%)
• Frequency of use at least weekly (97.4%)
• Severe episodes of vomiting with periodically recurring (cyclic) character (100%)
• Relief of symptoms with very hot bathing (92.3%)
• Periumbilical or epigastric pain (85.1%)
• Resolution of the syndrome after cessation of cannabis use (96.8%)
• Absence of other significant pathology capable of explaining the clinical picture.
Supportive characteristics:
• Age < 50 years
• Weight loss during episodes > 5 kg
• Symptoms occurring predominantly in the morning
• Intestinal transit unaffected.
According to Zimmer et al. (2019), the insurance expenditure per patient until diagnosis amounts to USD 76,920, whereas Perrotta et al. (2012) had previously estimated the cost at approximately USD 95,000.
Therapeutic considerations
From a therapeutic standpoint, antiemetic agents are usually ineffective. The antipsychotic droperidol appears to provide better results, whereas the most effective intervention is abstinence from THC. Abstinence from cannabis use is frequently resisted by patients, since most are dependent and many hold the firmly established belief that cannabis use cannot be harmful, while medical recommendations to the contrary are often perceived either as prejudice or as ignorance.
Cannabis is frequently used by patients suffering from CVS because it normally alleviates symptoms: agonists of CB1R reduce the tendency toward vomiting through a central mechanism that also involves serotonergic receptors. With regard to hot bathing, the transient improvement it produces has often been regarded as strongly suggestive of CHS. However, approximately half of patients with CVS also report symptomatic relief with this method; therefore hot bathing cannot be considered pathognomonic for CHS.
Etiopathogenetic considerations
The etiology and pathogenesis of CHS remained obscure until recently, and numerous evidently unfounded hypotheses had been proposed. Russo et al. (2021) clarified the issue to a large extent through the identification of a group of genetic polymorphisms closely associated with the syndrome: mutations in the genes CYP2C9, COMT2, DRD23, TRPV1, and ABCA14. On the background of these polymorphisms, cannabis abuse induces downregulation of CB1R, thereby impairing the capacity to suppress the tonic activity of the vomiting reflex. Temporary relief appears to arise through recruitment of TRPV1 and its sensory connections with the hypothalamus, which, as a thermoreceptor, becomes stimulated during very hot bathing.
From our clinical experience with patients requiring cannabis as medication in high doses, CHS does not appear to be a concern. It seems that abuse of THC without adequate counterbalance—at least by CBD (as is typically the case with type I cannabis, preferred by recreational users)—plays a decisive role in the manifestation of CHS, naturally in combination with the genetic background described by Russo et al. (2021).
CHS is essentially a clinical entity encountered in Emergency Departments and concerns primarily recreational users. It is generally a diagnosis of exclusion and, as noted above, imposes considerable costs on healthcare insurance systems before the diagnosis is established. These costs arise from investigations aimed at excluding other conditions and from repeated hospitalizations. When one also considers that such patients commonly present to hospitals more than ten times per year before diagnosis is made, the economic burden becomes substantial, with a tendency to increase further as recreational use becomes more widely legalized. It has also been reported that the number of patients presenting with persistent vomiting had increased by 17.9% by 2017 compared with 2009, the year when liberalization of recreational use began (Al-Shammari et al., 2017). The largest case series was published in 2012 by Simonetto et al. (2012) and included 98 patients.