B.2. Properties of “minor” phytocannabinoids
Current knowledge concerning the pharmacological properties of most minor cannabinoids remains limited. Some of these compounds do not yet even possess an established name and are referred to only by a provisional code. The properties of the most common among them that are generally accepted, as noted above, are the following:
B.2.1. Cannabigerol, CBG
CBG, with a molecular weight of 316.5, although displaying chemical affinity for CB1/2R, lacks significant agonist potency. Nevertheless, it modulates signaling mediated by CB1/2R and their heterodimers even at low concentrations (0.1–1 μM), because it influences downstream signaling pathways through additional mechanisms. Assays measuring cAMP activity, pERK activation, and β-arrestin recruitment have shown that CBG is a partial agonist of CB2R, with efficacy lower than that of the endocannabinoids, and a weak agonist of CB1R without clinically significant psychotropic activity [Zagzoog et al., (2020), Caprioglio et al., (2022)]. In cells expressing CB1R, CBG preferentially facilitates biochemical pathways activated through the Gi fraction and therefore inhibits signaling dependent on cAMP. The action observed in cells expressing CB1–CB2R heterodimers resembles that observed in cells expressing CB2R alone. Taking into account the totality of the in vitro experimental data, a convincing case cannot be made for an allosteric action of CBG on CB1R, since such an interpretation would not explain the Gi-mediated signaling observed. An alternative interpretation is that CBG behaves as a polymorphic agonist exhibiting selective agonism at the classical cannabinoid receptors (Navarro, Varani et al., 2018). Some downstream signaling pathways dependent on CB1/2R and presumed to be modified under the influence of CBG are illustrated in Figure 7a of Chapter 3.
In contrast to all other cannabinoids, CBG acts as a strong α2-adrenergic agonist at low concentrations. This property has been proposed as a possible explanation for beneficial effects reported in autism and attention-deficit disorders (Cascio et al., 2010).
CBG also acts as an antagonist of the serotonergic receptor 5HT1A (Cascio et al., 2010), where it counteracts the action of CBD and CBDa. For this reason caution is required in situations involving nausea and vomiting, and also in several other contexts. For example, antagonism of CBG at 5HT1A could theoretically exacerbate anxiety or psychosis-like manifestations that may occasionally occur after administration of high doses of THC, oppose CBD treatment intended to control alcohol consumption, and attenuate the antipsychotic action of CBD.
CBG is furthermore an agonist of TRPV1, TRPV2, TRPV3, TRPV4, and TRPA1 receptors at low concentrations, and an antagonist of TRPM8 (De Petrocellis et al., 2011). Antagonism of CBG toward TRPM8 occurs at concentrations of approximately 110–160 nM, which are readily achievable clinically. Indeed, CBG appears to be the most potent antagonist of TRPM8, a receptor known for its pathogenetic association with several neoplasms (Liu Zhaoguo et al., 2016). For conditions in which such preclinical indications exist, the idea of conducting clinical studies is therefore becoming increasingly compelling. A representative example is androgen-sensitive prostate cancer: TRPM8 antagonists inhibit calcium influx–induced proliferation and invasive behavior in prostate neoplasms expressing androgen receptors (AnR). This effect also applies to neoplasms resistant to pharmacological castration, whereas the behavior of AnR-negative cancer cells is not affected (Di Donato et al., 2021). In this context CBG appears to represent a promising and feasible therapeutic candidate, since other inhibitors currently under investigation remain far from approval for clinical use.
CBG also exhibits neuroprotective properties (Nachnani et al., 2021), while increasing importance is attributed to its function as a dual PPARα/γ agonist for the management of dyslipidemias and cancer (D’Aniello et al., 2019).
The antimicrobial properties of CBG, studied extensively by Farha et al. (2020), acquire particular significance at a time when new antibiotics are not being developed and multidrug-resistant bacteria have become a serious threat to public health. Moreover, since CBG can be synthesized easily and inexpensively in the laboratory from olivetol and geraniol, it may eventually prove useful even in situations requiring relatively high concentrations. CBG strongly inhibits Gram-positive bacteria, suppresses biofilm formation, eradicates preformed biofilms, effectively eliminates bacteria in the dormant state, and makes the development of resistance extremely difficult (Aqawi et al., 2021).
More specifically, the mean MIC90 of CBG against 96 clinical isolates of MRSA was determined to be 4 μg/mL (12 μM), with a range of 2–8 μg/mL (6–24 μM) in the study by Farha et al. (2020), whereas the lower limit of this range was found to be 1 μg/mL in the study by Appendino et al. (2008) (see above). Such concentrations are achievable in tissues following administration of relatively high oral doses; however, since CBG does not display psychotropic activity, it could potentially be evaluated, possibly also in combination regimens. For superficial suppurative infections these concentrations are easily attainable. For example, CBG in a 15% oil preparation corresponds to a concentration of 477 mM—approximately 120,000 times greater than the mean MIC90 required. In the case of resistant Gram-negative bacteria such as E. coli, K. pneumoniae, and P. aeruginosa, which are not sensitive to CBG because the outer cell membrane is impermeable (very high MIC values on the order of 65 μM), the observed synergy with polymyxin B is particularly noteworthy for difficult clinical situations. Farha et al. (2020) report, for example, suppression of a resistant E. coli strain using 3 μM CBG combined with a subactive concentration of polymyxin B (0.062 μg/mL). The relationship of CBG with various receptors is presented in Table 17.
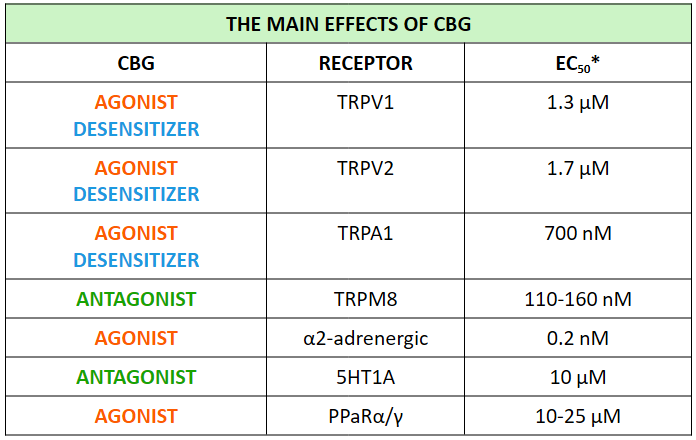
Table 17. The relationship between CBG and various receptors (Calapai et al., 2022) Data compiled from studies by Cascio et al. (2010), De Petrocellis et al. (2011), Ruhaak et al. (2011), Borrelli et al. (2014), etc. *Concentrations below 5 μM are considered easily achievable with oral administration of CBG, but 5-10 μM is not unattainable.
In the management of intraocular hypertension/glaucoma, CBG appears to claim a potential role, since the alternative cannabinoid-based options—namely THC and CBN—are associated with undesirable adverse effects, both ocular (hyperemia and conjunctival redness) and central nervous system effects. With regard to efficacy in reducing intraocular pressure, CBG appears to surpass CBN during chronic administration, according to the earlier study of Colasanti, Craig, & Allara (1984). A practical limitation, however, is the absence of pharmaceutical formulations suitable for ophthalmic use.
The antineoplastic properties of CBG were reported relatively early by Baek et al. (1996 & 1998) and continue to be investigated (Ligresti et al., 2006). These effects partly parallel its anti-inflammatory properties: partial agonism at CB2R, activation of vanilloid receptors and PPARγ, and antagonism at TRPM8 [De Petrocellis et al., (2011), Cascio et al., (2010), Ruhaak et al., (2011)]. In summary, CBG induces apoptosis, promotes the generation of reactive oxygen species in malignant cells, upregulates the protein CHOP1, and inhibits proliferation of cancer cells, at least in the colon. These actions appear to be confirmed in animal models (Borrelli et al., 2014). When co-administered with other cannabinoids—for example CBD—antineoplastic effects appear to be enhanced in leukemia (Scott et al., 2017, in vitro study). Anorexia and cachexia in patients with neoplastic disease or AIDS also appear to improve with CBG, similarly to the effect observed with THC (Brierley et al., 2017 & 2019). According to the same authors, full-spectrum CBG extracts appear to be superior to the isolated compound, an observation consistent with the general experience concerning cannabinoids in all medical applications. Particularly noteworthy is the more recent recognition of a possible role for CBG in the management of glioblastoma multiforme [Scarlett et al., (2018), Lah et al., (2021)].
Preclinical evidence suggests that CBG exerts protective effects on the cellular components of the blood–brain barrier (microvascular endothelial cells, pericytes, and astrocytes) under conditions of oxygen and glucose deprivation. At a concentration of 3 μM, CBG reduced levels of lactate dehydrogenase (LDH) in blood–brain barrier cells, a finding that reflects reduced reliance on anaerobic glycolysis and diminished conversion of pyruvate to lactate in hypoxic cells under the influence of CBG.
CBG also reduced the release of IL-6 and the levels of proteins associated with DNA damage. Using appropriate antagonists, the participation of CB1, CB2, PPARγ, PPARα, 5HT1A, and TRPV1 receptors in the mechanism responsible for the reduction of LDH was investigated and excluded. At present, no molecular target has yet been identified that could explain this particular action of CBG (Stone, England, & O’Sullivan, 2021).
In an experimental animal model of inflammatory bowel disease developed by Borrelli et al. (2013), CBG demonstrated both preventive and therapeutic effects at different injectable doses: 1 and 5 mg/kg respectively. The therapeutic action of CBG consisted in its ability to restore the integrity of the intestinal epithelium, accompanied by reduced infiltration by neutrophilic leukocytes. It also included a reduction in epithelial dysplasia, associated with decreased levels of inflammatory cytokines and reduced expression of iNOS, although not of COX, whose inhibition appears to require much higher doses (Ruhaak et al., 2011).
In cutaneous inflammation, CBG behaves as a transcriptional repressor of genes promoting DNA methylation of the keratin-10 gene. It appears capable of regulating cellular proliferation and differentiation, thereby representing a compound potentially useful in the treatment of acne (Pucci et al., 2013).
From a pharmacokinetic standpoint—and although it has not yet been fully studied in humans—CBG behaves similarly to other phytocannabinoids. After a single oral administration, its half-life ranges between 2 and 6 hours. It is also detectable in the brain. CBG is metabolized in the liver, with the predominant pathway being allylic hydroxylation by CYP450 monooxygenases, primarily CYP2J2. The principal metabolites are monohydroxy compounds. Like other cannabinoids, CBG is excreted in the form of glucuronides (Calapai et al., 2022).